(osmosis.org)
You’d have to be living in a cave on Mars to not have heard anything about the Zika virus epidemic sweeping through South America or it’s link to a dreaded birth defect: microcephaly. But as with every news worthy epidemic, there’s a lot of fear and plenty of misinformation. Fear is natural to something as terrifying as thousands of cases of birth defects linked to a virus that few people have ever heard about until a few months ago, but fear must not cloud our judgment and lead us to claim this or that about the virus without support of the facts. Stop and take a deep breath. Zika is indeed terrifying but like every other disease, science can help us understand what it is, what it does, and most importantly, how to stop it.
Unfortunately, the Internet can be a breeding ground for terrible ideas and conspiracy theories. Just as a quick spoiler on the following conspiracy theories : 1) Zika is not caused by or spread by genetically modified mosquitoes, 2) the epidemic did not occur because of tests with a Zika vaccine, and 3) while it cannot be ruled out entirely, larvicides/pesticides are not responsible for microcephaly (more discussion on these conspiracy theories later).
There’s a lot we still don’t know about the virus still but there’s a lot we have learned already and new information is emerging every day. We must be cautious: as members of a supposedly intelligent democracy, we must be careful to not over exaggerate or underestimate this problem—we must look at the facts and draw our conclusions from there.
Recently I’ve prepared a report on the Zika virus for an outside project, which required a great deal of reading scientific papers, news articles, reports from public health organization, listening to podcasts on the virus, and seminars discussing the most recent findings on it.
I present here, to the best of my ability, the most up-to-date, scientifically verified information about the Zika virus, what we know and don’t know about the risks it poses, and debunking some of the misinformation around it. At the end I make a few suggestions about what should be done about it. I include a glossary of important terms as well as references to important papers on the zika virus.
This post is really long (probably my longest blog post ever) so feel free to skip to whichever topic about the virus you are most interested in. Here’s links to the different topics:
What is it?

Viral entry into a cell. (wikipedia.org)
Zika is a virus that was discovered in the Zika Forest in Uganda in 1947 [1]. Scientists were looking for other types of viruses and discovered it by chance when one of the test monkeys became ill with something previously unknown.
Zika is a flavivirus, a family of viruses that includes dengue, chikungunya, yellow fever, and West Nile.
Like other viruses, Zika invades specific cells, hijacks those cells in order to force the cell to copy its DNA and make more viral particles.

Viral replication (wikipedia.org)
The reason why Zika is such a problem compared to other flaviviruses like dengue (which is far more common) is that is has been linked to a devastating birth defect, microcephaly (more on this later).
On February 1, 2016 the World Health Organization (WHO) has declared Zika virus a Public Health Emergency of International Concern. The Centers for Disease Control (CDC) in the United States has also issued a travel advisory to pregnant women considering visiting countries with ongoing Zika outbreaks has released guidelines for health care providers in the US who are treating pregnant women whom may have traveled to an area with Zika virus [2, 3].
Where did it come from?
While it may have been discovered in 1947 [1], it’s been spreading slowly across Africa since then. A distinct Asian variety of the virus was first discovered in 1966 in Malaysia [4]. The first epidemic of Zika occurred in the Micronesian island of Yap in 2007. Since then it has spread across the Pacific including an epidemic in French Polynesia in October 2013 to April 14. The virus spread to Easter Island off the coast of Chile sometime after that and the first cases in Brazil were reported in February 2015.
We know how the virus spread because over the years, scientists have collected viruses from various parts of the word, analyzed the viral DNA and RNA, and compared the results [5]. We know that the virus in the Americas is related to the Asian variety.
Zika outbreaks have been reported in 52 countries, included 31 in the Americas. More recently out breaks in Indonesia and Malaysia have also been reported.
No cases of mosquito-spread Zika have occurred in the US. (When a disease is spread by the an organism that carries it in a place in which that organism lives, we call that autochthonous transmission. Autochthonous transmission of Zika virus in the US would mean that a case occurred because of a mosquito bite. A non-autochthonous case of Zika would be someone traveling to a country with Zika, getting bitten by a Zika-carrying mosquito, then returning home and being diagnosed). So far, the only cases of Zika in the U.S. have been 1) people that traveled to regions in virus outbreaks or 2) a few cases of sexual transmission.
How is it spread?
Zika is spread through bites of the common mosquito Aedes aegypti, a species that bites during the daytime, but it can potentially be spread by any mosquito of the Aedes genus, including the Asian Tiger mosquito (Aedes albopictus), and many other species. Aedes mosquitoes also carry the other flaviviruses (dengue, chikungunya, yellow fever, and West Nile).

Aedes aegypti mosquito (commons.wikimedia.org)
Aedes aegypti mosquitoes are common to most of Central and South America as a well as 12 states in the South Eastern United States. However, Aedes albopictus can be found in 30 states, including along the entire Eastern seaboard [6].
Keep in mind that differences in the USA and Brazil means that the spread of mosquito-borne disease like Zika will also be different. For example, many people in South America don’t have access to running water, which means that water is stored in containers outside, which make perfect breeding ground for Aedes mosquitoes. Also, many people don’t have air conditioning so they do not stay indoors and unexposed to mosquito bites.
That being said, it is very possible that Zika will spread with the US [7] and we may see local outbreaks but almost certainly nothing compared to what’s happening in Brazil (see below for more).
*It should also be noted that Aedes mosquitoes are widely distributed throughout the globe but studies predict even greater distribution, meaning more areas for mosquito-borne diseases to spread. This is an often forgotten consequence of climate change. As the globe warms and certain regions warm, mosquito spread is predicted to increase, and the disease they carry along with them. [8, 9]*
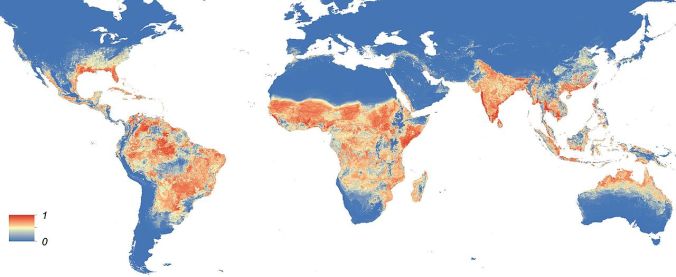
Global distribution of Aedes aegypti mosquitoes (commons.wikimedia.org)
Can Zika be spread through sex?
Yes, there have been two confirmed reports of sexual transmission occurring in the US and the CDC is currently evaluating a potential 16 more. What this means is that a person traveled to a Zika-containing country, got bit with a Zika mosquito, returned home and had sex with his partner, and the virus was detected in the partner. The virus has also been detected (by RT-PCR) in semen long after the infection has passed and the virus has been cleared from the blood [10]. Men infected with the virus are definitely at risk of passing it to their partners.
What is the risk of a Zika outbreak occurring in the United States?
The risk of outbreaks of Zika occurring in isolated pockets in the US, especially in states such as Texas or Florida (where mosquitoes can breed year round) is likely [7]. However, it is very unlikely that the epidemic proportions we are seeing elsewhere will occur in the US. For example, Dengue outbreaks have been occurring for years in Brazil and other nations in South America but there has never been a Dengue outbreak in the continental US (Dengue is also spread by Aedes mosquitoes). One exception is a Dengue outbreak did occur in Key West in 2009/10 but this is a semi-tropical environment more comparable to Central/South America than the rest of the South Eastern US.
Another example is the West Nile virus outbreak in the late 1990s/early 2000s, another mosquito-borne flavivirus. However, while West Nile may be in the same viral family as Zika, their biology and transmission patterns are quite different. For example, viruses like Zika and dengue require sufficient quantities of virus to build up in their host (e.g. humans) in order for a passing mosquito to pick up the virus and spread it to the next host. For West Nile, while it can infect humans, its host reservoir is primarily birds. This allowed mosquitoes to bite birds, get infected to the virus, and pass it along to humans. Therefore, a continuous cycle can exist for West Nile because birds obviously don’t practice mosquito bite prevention. With humans living in the US, our exposure to mosquitoes is much less so the risk of perpetuating cycle developing that would drive a Zika epidemic is unlikely to occur.
Finally, the differences in lifestyles and economic circumstances of the different populations mean that Americans are less exposed to mosquitoes and thus less likely to be bitten (see above).
In conclusion, will we see autochthonous (mosquito-spread) Zika cases in the United States? Probably. Will it be an epidemic that impacts the whole country? Probably not.
Thankfully the CDC is already issuing guidelines for the detection of the virus in pregnant women that may have traveled regions with virus and taking all the necessary steps to help control the virus in the US. And of course, the best strategy to prevent the spread of Zika to the US is to help Brazil and other Central and South American countries in containing the ongoing epidemic.
What does it do?
Most Zika cases (about 80%) have no symptoms but those that do present with mild symptoms like fever, rash, and swelling lymph nodes. The difficult of diagnosing people infected with the virus (i.e. pregnant women) is one of the major problems health officials in South America are confronting. Work is being done to improve testing for the virus (see below)
The symptoms last for about a week and virus is cleared from the blood in about a month.
The real concern with Zika is that it may be the cause of the severe birth defect microcephaly and the nervous system disease Guillain-Barre syndrome (See below).
How bad is the epidemic occurring in Brazil and other countries in the Americas?
Unfortunately, this question is difficult to answer because 1) Zika virus is notoriously difficult to detect and distinguish from other flaviruses (see below) 2) direct detection of the virus can is only possible between 7-10 days of the infection 3) symptoms of the virus are similar to other flaviviruses and 4) most cases are asymptomatic (no symptoms at all).
 Nevertheless, as of February 5, 2016 the WHO reported 26 countries have reported Zika outbreaks (this number has been increased to 31 as of March 11). Also, the Brazillian Ministry of Health reported that virus has infected between 500,000 and 1.5 million people. Because the virus is so difficult to diagnosis, the actual number of cases is probably much higher than this.
Nevertheless, as of February 5, 2016 the WHO reported 26 countries have reported Zika outbreaks (this number has been increased to 31 as of March 11). Also, the Brazillian Ministry of Health reported that virus has infected between 500,000 and 1.5 million people. Because the virus is so difficult to diagnosis, the actual number of cases is probably much higher than this.
Zika cases have been reported in 26 countries in the Americas including Mexico and Puerto Rico. Colombia is reporting the second highest number of zika cases at about 20,000.
The full impact of this large number of cases and its implications for microcephaly in Brazil, Colombia, and other countries is unknown but I’ll discuss that shortly.
How is Zika virus detected in a human patient?
When a virus invades a host organism, the host’s immune system launches an attack against the virus. Part of this response involves the generation of specific antibodies to target and clear the virus from the body. Using serological assays, these antibodies can be detected from the serum (the blood minus blood cells and clotting factors). However, because Zika, dengue, and other flaviruses are closesly related, antibodies that detect one seem to detect them all. This makes serological testing somewhat unreliable because you don’t know for sure if a positive result menas Zika, dengue, chikungunya, etc.

Functions of antibodies in the immune system

Example of RT-PCR results
A more reliable test is for the specific genetic material of the virus itself. A very common experimental technique called RT-PCR (see the glossary) is able to distinguish the genetic material of Zika from other flaviruses [11, 12]. However, this has it’s own problems because the virus can only be detected this way from blood within 7-10 days after infection. After this 10-day window, the virus is cleared from the blood by the immune system.
RT-PCR is also useful for detected the virus in other tissues and so far Zika virus genetic material has been found in semen, breast milk, the placenta, amniotic fluid, and brain tissue of infants diagnosed with microcephaly.
Improved serologic testing is required because antibodies can persist for a very long time while RT-PCR needs to be done immediately.
Does Zika cause microcephaly?
This is the million-dollar question when it comes to Zika and the greatest source of concern about the virus.
Microcephaly is a medical condition defined by an abnormal brain development which results in a small head. According to Wikipedia, “people with the disorder have an intellectual disability, poor motor function, poor speech, abnormal facial features, seizures, and are short.” Microcephaly is a severe birth defect and it is not uncommon for infants with the condition to die at birth or shortly after. It’s causes are poorly understood. No treatments exist for microcephaly.
It is this concern over microcephaly that has prompted the WHO to declare the virus a public health emergency and the prompt the CDC to issues its travel advisory [13]. Dengue virus is far more prevalent than Zika but dengue infections are only rarely fatal (about <1% of infected individuals that receive proper treatment). The striking rise in microcephaly during the time of Zika epidemic has made it clear the Zika virus is an illness that needs to be taken extremely seriously.

Microcephaly compared to normal (wikipedia.org)
However, there is a lack of conclusive scientific evidence that Zika virus infections directly (key word!) cause microcephaly. Importantly, there is a multitude of indirect evidence that strongly suggests that Zika is the culprit. I’ll spend a little time going through what it is we know for sure.
There are some problems with the numbers. First, diagnosis of microcephaly can be difficult [14]. In the most general definition microcephaly is diagnosed head size two standard deviations small than (this means a head size smaller than 95% of births). Microcephaly can also be dtected by ultrasound in the developing fetus in the womb. Between mid-2015 and Jan 30, 2016, the Brazilian Health ministry reported some 4,783 cases of microcephaly. 1,103 cases have completed a rigorous clinical analysis. 404 cases have been confirmed as suffering from microcephaly and 709 cases have been discarded (not microcephaly) but 3,670 cases still need to be evaluated [14]. The yearly average for microcephaly in Brazil is around 150 so clearly there’s already a large increase in microcephaly cases. Cases of microcephaly are also under investigation in Colombia, the country second hardest hit by the virus.
Also, the CDC reported the first case in the US of brain damage in a baby that has been linked to Zika.
Some experts have suggested that the number of microcephaly cases has actually been overestimated. They argue that microcephaly prior to the epidemic is much lower when compared to the US and Europe, which suggests those baseline numbers were under-reported. But now, all of a sudden, health officials are paying close attention, which may be artificially inflating the numbers.
That being said, we’re still looking at at least a 5-20 fold increase in microcephaly cases. The association between microcephaly and the Zika epidemic still seems like a strong association in my book and a real problem (evidently the WHO and CDC do too).
Just to summarize all of this, we can reasonably conclude that there is a significant increase in the number of microcephaly cases that has coincided with the onset of the Zika epidemic. However, additional prospective data is required to confirm these numbers. Besides the number of cases, there’s also a lot of laboratory work that points the finger squarely at Zika. I’ll go through these findings next.
What is the scientific proof that Zika virus causes microcephaly?
 As I alluded to above, the only way to prove definitively that Zika causes microcephaly is to run a large, prospective study in which pregnant mothers who have confirmed Zika infection are examined and followed for their entire pregnancy, other factors like diet, genetics, and environment are excluded, the incidence of microcephaly and other birth defects recorded, and compared to pregnancies without Zika infection. If there’s a significant increased in microcephaly in the proven Zika cases, then we can reasonably conclude that Zika is is the most likely culprit (though even this study would not prove 100% causality). In order for to be done successfully, a very large number of people would be required to participate in the study. Fortunately but really unfortunately, the ongoing epidemic provides a large data set to work with. However, patients would need to be identified, diagnosed, and followed for their entire pregnancy which would require a ton of work and money. Concluding a study like this could take a year or longer and would require a huge concerted effort but local doctors, patients, and public health officials. I’m sure a study like this is already being planned and data is probably being collected as I write this. In fact, some small scale prospective studies have already been done (see this paper for a great summary of the various findings from different studies [15]).
As I alluded to above, the only way to prove definitively that Zika causes microcephaly is to run a large, prospective study in which pregnant mothers who have confirmed Zika infection are examined and followed for their entire pregnancy, other factors like diet, genetics, and environment are excluded, the incidence of microcephaly and other birth defects recorded, and compared to pregnancies without Zika infection. If there’s a significant increased in microcephaly in the proven Zika cases, then we can reasonably conclude that Zika is is the most likely culprit (though even this study would not prove 100% causality). In order for to be done successfully, a very large number of people would be required to participate in the study. Fortunately but really unfortunately, the ongoing epidemic provides a large data set to work with. However, patients would need to be identified, diagnosed, and followed for their entire pregnancy which would require a ton of work and money. Concluding a study like this could take a year or longer and would require a huge concerted effort but local doctors, patients, and public health officials. I’m sure a study like this is already being planned and data is probably being collected as I write this. In fact, some small scale prospective studies have already been done (see this paper for a great summary of the various findings from different studies [15]).
However, what data exists right now?
As I described above, the drastic increase in microcephaly (even if it may be over reported) coincides with the start of the epidemic and cannot be ignored. This is fairly solid associative evidence, even if it doesn’t prove a direct cause.
Some have argued that there were no incidences of microcephaly in the French Polynesia outbreak of 2014 but in fact, once the Brazil numbers started to be released, health authorities reported they had identified an increase in microcephaly cases but did not publicize the results (perhaps because they thought it was unrelated or didn’t have strong enough data). Also, there was an increased number of abortions during the outbreak (abortion is legal in French Polynesia where it illegal in Brazil) which suggests an increased rate of birth defects in developing fetuses. As of March 11, 2016 the WHO reports that only Brazil and French Polynesia have reported an increase in microcephaly cases but cases in Colombia are currently under investigation.
We also have a strong pool of data about the detection of the virus. The Zika virus genetic material has been detected in semen, breast milk, the placenta, the amniotic fluid, and the brains of babies that were born with microcephaly and died shortly after [10, 16, 17].
What’s amazing (and terrifying) is the detection in the placenta, amniotic fluid, and brain tissues. The placenta has numerous roles in protecting the fetus such as a source of nutrients as well as a quite impermeable protective barrier. Very few viruses (such as the TORCH pathogens) can cross the placenta and that fact that Zika has been detected not only in the placenta but also the amniotic fluid and brain tissues, strongly suggests that virus can indeed cross the placenta and infect the brain of the developing baby.
The most striking and scientifically strong piece of evidence comes from a paper released in the New England Journal of Medicine, the top clinical journal in the world [12]. Keep in mind it is only a single case study but provides probably the most thorough analysis of a microcephaly case.
 The background behind the patient is a European woman who was 13 weeks pregnant (1st trimester) traveled to Brazil in February 2015 (the start of the epidemic) and displayed symptoms of the Zika virus (though it was not diagnosed as Zika at the time). She returned to Europe but around 26 weeks into her pregnancy (3rd trimester), an ultrasound revealed severe abnormalities in the brain of the fetus, including microcephaly. The woman and her doctor decided an abortion was the best option and the fetus was analyzed post mortem. The scientists found Zika virus in the brain of the fetus and only the brain (no other organs). Importantly, the entire genome (the total amount of genetic material unique to a particular virus) was recovered. This is important because this proves that only Zika, and not any of the other flaviruses, was detected. Furthermore, in addition to microcephaly, the brain has numerous other abnormalities such as calcification. Finally, using a high-powered microscopy technique called electron microscopy, the physical virus itself was detected in the brain tissue.
The background behind the patient is a European woman who was 13 weeks pregnant (1st trimester) traveled to Brazil in February 2015 (the start of the epidemic) and displayed symptoms of the Zika virus (though it was not diagnosed as Zika at the time). She returned to Europe but around 26 weeks into her pregnancy (3rd trimester), an ultrasound revealed severe abnormalities in the brain of the fetus, including microcephaly. The woman and her doctor decided an abortion was the best option and the fetus was analyzed post mortem. The scientists found Zika virus in the brain of the fetus and only the brain (no other organs). Importantly, the entire genome (the total amount of genetic material unique to a particular virus) was recovered. This is important because this proves that only Zika, and not any of the other flaviruses, was detected. Furthermore, in addition to microcephaly, the brain has numerous other abnormalities such as calcification. Finally, using a high-powered microscopy technique called electron microscopy, the physical virus itself was detected in the brain tissue.
While it’s not exactly a smoking gun (scientists can be very difficult people to convince…), this study strongly suggests that the Zika virus caused the microcephaly and other brain defects in this particular case. However, other cases are required to confirm this important (and frightening!) finding.
It’s also important to note that compared to the total number of cases of Zika infection, the incidence of microcephaly is relatively low. That being said, any increases in this devastating birth defect caused by Zika are too many and must be taken extremely seriously.
If want to learn more, check out this other blog post provides another great summary of all the data.
Does Zika cause Guillain-Barre Syndrome?
Guillain-Barre syndrome (GBS) is a serious illness that can result in paralysis, permanent disability, or death. GBS is caused by a hyper-reactive response of the immune system that results in the bodies own immune defenses attacking the nerves that control movements. Certain types of infections, including other flaviviruses such as dengue and West Nile, can instigate this type of unexpected attack by the immune system. Therefore, it’s not unexpected that Zika may also been linked to the disorder.
An increased incidence of GBS was first reported during the outbreak in French Polynesia in 2014 [18] and a surge in cases has also accompanied the epidemic in Brazil [15]. A recent study [19] confirms that Zika is most likely cause of the surge of GBS cases that occurred during the French Polynesia outbreak, but the results are not conclusive. The incidence is relatively rare (about 0.24/1000 cases) [18] but at the scale of a country the size of Brazil, the number of GBS cases could be very large indeed.
How is it treated?

Dead mosquitoes
Unfortunately, there are currently no treatments or vaccines for Zika virus. The best method for treating the virus is prevention (see below).
Several groups are working on a vaccine but it would take years for a final product to be rigorously tested and widely distributed. A vaccine does represent the most long-term strategy to contain Zika and Anthony Fauci, director of the National Institute of Allergens and Infectious Disease (NIAID) predicts a vaccine will very likely be developed.
What can be done right now?
The best way to help keep Zika from spreading to the US is to help Brazil and other countries in the Americas to contain the Aedes mosquito population and prevent mosquito bites.

Mosquito netting (commons.wikimedia.org)
Mosquito bite prevention is easy and cheap but as I described above, can be difficult in rural and underdeveloped communities in South America. Aedes mosquitoes primarily bite during the daytime but in the United States, we take for granted things like screen doors and the ability to take refuge from hot days by staying indoors with our air conditioning. But many people in South America don’t have these amenities and are constantly exposed to outside air and thus susceptible to mosquito bites. However, distribution of things like mosquito repellent and mosquito netting treated with repellent are cheap and easy opportunities to help limit bites of mosquitoes. If outdoors, wearing long-sleeves to reduce the amount of exposed skin is another common-sense way of limiting mosquito bites. However, in hot climates, this strategy may not not sound very appealing.
Another problem is the lack of indoor plumbing in many rural areas in South America which means water is stored in open containers. Efforts should be made to help protect these water sources and attempt to clear them of mosquito larvae (i.e. treatment with tested larvicides to kill the mosquitoes in their adolescent stage).
As a long term strategy, the mosquito population must be controlled and this has been attempted in many ways from spraying with harmful pesticides, to treating exposed water with larvicides, to even introducing certain species of fish that thrive on (this review covers many of these attempts to control the mosquito population). Unfortunately, Aedes aegypti mosquitoes need only a tiny amount of water (even that found in soda bottle lid) in order to breed. Thankfully many of these efforts are cheap but require a coordinated effort, especially at the local level. Other more advanced strategies, such as introduction of genetically modified mosquitoes to limit the growth of the mosquito population may represent new alternatives (I’ll discuss this new technological advancement in a future blog post because it’s actually pretty cool).
A recent article by Brazilian public health authorities and published in the Journal of American Medical Association made several recommendations to fight the virus [20]. I summarize the six points here.
- Increased gathering of epidemiologic data on the virus and research into the consequences of its infection.
- Development of a fast and reliable serological test for Zika
- Control of the Aedes aegypti population
- Define standardized protocols for treatment of Zika infection.
- Development of a vaccine.
- Improve the health care system to properly address the epidemic.
These six recommendations are not small tasks but would require a great deal of effort but touch on many of the points I’ve already made about the virus, what we don’t know, and what we need to fight it.
Why is it some new epidemic seems to keep happening, almost out of nowhere?
You probably remember that in 2014 that world was stricken with panic of a far more deadly and horrific virus (though less infectious): Ebola. Similar to Zika, an epidemic spread throughout a region of the world and few isolated cases reached the U.S. Despite significant failures that undoubtedly cost hundreds or even thousands of lives (the WHO was slow to mobilize an international response compared to Zika), that epidemic was eventually contained.
Now we have Zika and a similar pattern is emerging. This time public health agencies are taking it much more seriously and responding quickly, at least when compared to Ebola.
Zika and Ebola have other things in common too. 1) both viruses have been known about for years but were relatively minor global problems 2) they spread incredibly quickly in a particular region.
I want to speak a bit about this second point. How could this have been allowed to happen? If an Ebola or Zika epidemic started in the US, would we have the same type of problem that we are seeing in less developed nations?
One argument is that the failure of local health systems and absence of coordinated public health efforts at the local, regional, national, and international efforts have resulted in the rapid spread of the disease. The failure to coordinate an international effort to help provide aid and support to African nations certainly exacerbated the Ebola epidemic. But with Zika, because it is so difficult to diagnose and it is spread so easily by mosquitoes, this argument doesn’t necessarily hold water. One thing is clear though, an improved international system needs to be put in place to closely monitor emerging diseases. We knew Zika was spreading since the Yap Island outbreak in 2007 but no one could have anticipated the explosion of the virus in Brazil, or the link in microcephaly. The virtual lack of research about Zika undoubtedly contributed to this problem as well. There is no easy answer why outbreaks like Ebola and Zika happen.
Just as a contrast, let’s look at how the HIV virus took the US by surprise. Why did it become an epidemic? One reason may be that governmental leadership (i.e. the Reagan administration) completely ignored it for years despite scientists and public health experts raising the red flags. I won’t say anything more than that, but clearly public health failures can occur in any nation, even “developed” ones. Lack of strong central authority to mobilize a response to a public health crisis inevitably makes the crisis worse. We saw it with HIV, we saw it with Ebola, and things are slowly changing with Zika (as I mentioned, both the WHO and CDC have responded very quickly to this crisis. To what effect remains to be seen…)
But what about the next “Zika”, the one we don’t know about yet?

Improvements in the global public health sector are clearly required in order to identify new emerging viruses, coordinate an international response, and quickly contain the new bug before it can become a much larger problem.
Dispelling myths about Zika virus.
As promised, I want to spend some time debunking some of the absurd myths about Zika that have been floating around the Internet.
Myth #1: Zika virus is caused and spread by genetically modified mosquitoes.
There are numerous things wrong with this. First, we know that the virus originated from the Zika Forest in Uganda in 1947. Second, we have tracked its spread through Africa and the Asian variety that has emerged in a series of outbreaks from Yap island in Micronesia in 2007 to French Polynesia in 2014 to Brazil in 2015. Third, while there is indeed an ongoing trial in Brazil using genetically modified mosquitoes (GMM) produced by the company Oxitec and with complete support of the Brazillian government , the strategy is intended to control the mosquito population and is actually extremely safe. The mosquitoes used in this trial are sterile males carrying a lethal gene: they breed with wild females, that breeding kills all the eggs they produce, and then the GMM male itself dies. Similar trials already occurred in Cayman Islands and Malaysia between 2009-2012. The trials were extremely successful in controlling the mosquito population (about 80-90% of the native population) [21]. In fact, the GMM strategy may be a powerful new tool to help control disease-spreading mosquito populations. There is zero evidence that GMM have anything to do with the current Zika epidemic or microcephaly. A piece in the New Yorker does a great job of dispelling this absurd myth.
Myth #2: The Zika epidemic and microcephaly is caused by a faulty Zika vaccine.
This falls in to the same type of fear mongering related to vaccines and autism (no such link exists). First, there is not even a Zika vaccine thus any reason why one would have even been tested before the epidemic began in early 2015. Second, for all the reasons I described above, we know where the virus came from and how it spread. Third, vaccines are one of the greatest successes in the history of medicine and have saved millions and millions of lives. There is no evidence anywhere that vaccines would possibly cause microcephaly.
Myth #3: Microcephaly is not caused by Zika but by the use of a dangerous larvicide pyriproxyfen.
Of all the three myths presented here, this one is the most plausible because pesticides and other chemical agents used to control pests can indeed have unexpected ecological and health risks. However, the arguments brought up by the Argentinian group making the claim, do not hold water. First, the location that the larvicide was being used is not consistent with the reports of microcephaly. Second, the usage of the chemical is also not consistent with rise of microcephaly cases. Third, all the evidence I described above showing that Zika is most likely the cause of the microcephaly. For all these reasons, experts largely dismiss the claims about the larvicide.
Check out the Mad Virologists post also debunking Zika myths or the New Yorker article.
Concluding Thoughts
Zika virus is a terrifying virus that is spreading like wildfire but I want to end with five final thoughts specifically for easily frightened Americans:
- The Zika virus should be treated seriously but not hysterically.
- The risk of a Zika epidemic the scope of Brazil’s occurring in the United States is extremely low.
- The link between Zika and microcephaly is strong though not scientifically conclusive.
- There is a great deal about the virus and the epidemic that is still unknown so pay attention to what the CDC has to say and don’t overreact to over-hyped stories on the news.
- For the people of South America, this is a real threat and just because the risk to America is low doesn’t mean that this a problem that Americans should ignore. Brazil and other nations need our help and the US should be leading the world in the fight against disease.
Glossary
Aedes: A genus of mosquitoes that carries flaviviruses such as Zika and dengue; includes the species Aede aegypti (the culprit in the current epidemic) and Aedes albopictus.
Antibody: A main defense produced by the immune system. An antibody recognizes a specific disease and marks that infectious agent so that other immune cells can kill it.
Autochthonous: indigenous to a region, in epidemiology, transmission of a disease by a vector in the region of an epidemic (rather than a case reported in a region that is not experiencing the epidemic).Virus: an infectious agent that invades a cell and hijack’s that cell’s molecular machinery to make more viral particles. Usually consists of a small amount of genetic material (DNA or RNA) encapsulated by a protein coat; the genetic material is how the virus hijacks the cell to make more of itself.
Autoimmune disease: A disease in which the body’s immune system attacks its own cells and tissues.
Flavivirus: the family of viruses that includes dengue, chikungunya, yellow fever, West Nile, and Zika.
Genetically Modified Mosquito: A mosquito that has had its DNA scientifically altered so that it can be used to control wild mosquito populations. Two general classes exists 1) mosquitoes that transmit a lethal gene to other mosquitoes or 2) mosquitoes that are resistant to being the host for a particular disease.
Immune System: An organism’s complete system used for the defense against disease.
Larvicide: A chemical compound used to kill an insect when it is in its juvenile, or larval stage.
Microcephaly: A medical condition defined by an abnormal brain development which results in a small head. Numerous neurological problems may result from the disorder, including compromised cognitive function and intellectual disability.
Mosquito-borne disease: a disease such as Zika, dengue, or malaria that is transmitted through mosquito bites.
Pesticide: A chemical compound used to kill insects that are either harmful or a nuisance.
RT-PCR: Reverse-transcriptase polymerase chain reaction. A common technique in molecular biology that is able to analyze a sample for the presence or absence or a specific DNA sequence. Useful in determining the molecular identity of a unknown biological sample. Most labs are capable of running RT-PCR, provided they have the proper reagents.
Serologic testing: Analysis of a serum, a component of blood minus, for specific antibodies that the immune system has generated against an invading virus or other pathogen.
Sexually transmissible: a disease that can be passed from one partner to another through sexual intercourse. However, this does not mean this the primary route of transmission for the disease.
Vector: any organism that can spread a disease, such as a mosquito carrying malaria or Zika, a tick carrying lyme disease, or even a dog with rabies or a human with the flu.
Viral Reservoir: The host animal in which the virus replicates itself to sufficient quantities that it can be spread to other hosts.
Virus: an infectious agent that invades a cell and hijack’s that cell’s molecular machinery to make more viral particles. Usually consists of a small amount of genetic material (DNA or RNA) encapsulated by a protein coat; the genetic material is how the virus hijacks the cell to make more of itself.
Selected References
- Dick GW, et al. Zika virus. I. Isolations and serological specificity. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1952;46(5):509-20.
- Staples JE, et al. Interim Guidelines for the Evaluation and Testing of Infants with Possible Congenital Zika Virus Infection – United States, 2016. MMWR Morbidity and mortality weekly report. 2016;65(3):63-7.
- Oduyebo T, et al. Update: Interim Guidelines for Health Care Providers Caring for Pregnant Women and Women of Reproductive Age with Possible Zika Virus Exposure – United States, 2016. MMWR Morbidity and mortality weekly report. 2016;65(5):122-7.
- Enfissi A, et al. Zika virus genome from the Americas. Lancet. 2016;387(10015):227-8.
- Faye O, et al. Molecular evolution of Zika virus during its emergence in the 20(th) century. PLoS neglected tropical diseases. 2014;8(1):e2636.
- Kraemer MU, et al. The global distribution of the arbovirus vectors Aedes aegypti and Ae. albopictus. eLife. 2015;4:e08347.
- Bogoch, II, et al. Anticipating the international spread of Zika virus from Brazil. Lancet. 2016;387(10016):335-6.
- Naish S, et al. Climate change and dengue: a critical and systematic review of quantitative modelling approaches. BMC infectious diseases. 2014;14:167.
- Medlock JM, Leach SA. Effect of climate change on vector-borne disease risk in the UK. The Lancet Infectious diseases. 2015;15(6):721-30.
- Musso D, et al. Potential sexual transmission of Zika virus. Emerging infectious diseases. 2015;21(2):359-61.
- Campos GS, et al. Zika Virus Outbreak, Bahia, Brazil. Emerging infectious diseases. 2015;21(10):1885-6.
- Mlakar J, et al. Zika Virus Associated with Microcephaly. The New England journal of medicine. 2016;374(10):951-8.
- Heymann DL, et al. Zika virus and microcephaly: why is this situation a PHEIC? Lancet. 2016;387(10020):719-21.
- Victora CG, et al. Microcephaly in Brazil: how to interpret reported numbers? Lancet. 2016;387(10019):621-4.
- Broutet N, et al. Zika Virus as a Cause of Neurologic Disorders. The New England journal of medicine. 2016.
- Calvet G, et al. Detection and sequencing of Zika virus from amniotic fluid of fetuses with microcephaly in Brazil: a case study. The Lancet Infectious diseases. 2016.
- Martines RB, et al. Notes from the Field: Evidence of Zika Virus Infection in Brain and Placental Tissues from Two Congenitally Infected Newborns and Two Fetal Losses – Brazil, 2015. MMWR Morbidity and mortality weekly report. 2016;65(6):159-60.
- Oehler E, et al. Zika virus infection complicated by Guillain-Barre syndrome–case report, French Polynesia, December 2013. Euro surveillance : bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin. 2014;19(9).
- Cao-Lormeau VM, et al. Guillain-Barre Syndrome outbreak associated with Zika virus infection in French Polynesia: a case-control study. Lancet. 2016.
- Barreto ML, et al. Zika virus and microcephaly in Brazil: a scientific agenda. Lancet. 2016;387(10022):919-21.
- Lacroix R, et al. Open field release of genetically engineered sterile male Aedes aegypti in Malaysia. PloS one. 2012;7(8):e42771.